
Get the free amerigroup appeal timely filing limit
Show details
Claim Payment Appeal Submission Form This form should be completed by providers for payment appeals only. Member Information: Member First/Last Name: Member Date of Birth: ? Medicaid Member Coverage:
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign amerigroup appeal form
Edit your amerigroup provider appeal form texas form online
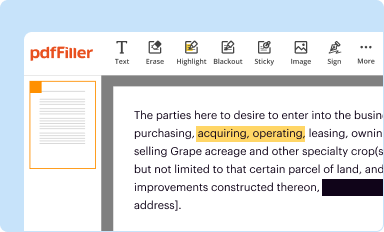
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
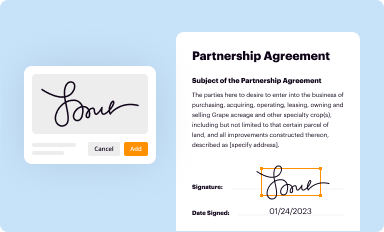
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
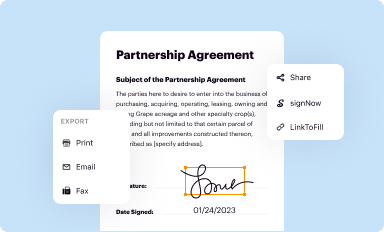
Share your form instantly
Email, fax, or share your amerigroup appeal mailing address form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing amerigroup medicare appeal form online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit amerigroup appeal form texas. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Create an account to find out for yourself how it works!
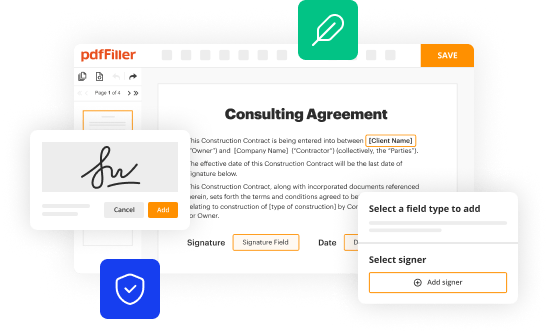
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out amerigroup provider appeal form
How to fill out Amerigroup appeal form?
01
Gather necessary information: Before starting to fill out the Amerigroup appeal form, make sure you have all the necessary information handy. This may include your personal details, policy number, claim details, reason for appeal, supporting documents, and any other relevant information.
02
Carefully read the instructions: It is important to carefully read and understand the instructions provided with the Amerigroup appeal form. This will ensure that you fill out the form correctly and provide all the required information.
03
Complete the personal details section: Start by filling out the personal details section of the Amerigroup appeal form. This typically includes your name, address, contact information, date of birth, and policy or member ID number. Provide accurate and up-to-date information.
04
Provide claim details: In the next section, provide the necessary information about the claim you are appealing. This may include the date of service, the healthcare provider's information, CPT or procedure codes, and any other relevant details. Be as specific and detailed as possible.
05
State reason for appeal: Clearly state the reason for your appeal in the designated section. Provide a concise and complete explanation of why you believe the initial decision or denial should be overturned. Support your reasons with facts, documentation, and any relevant evidence.
06
Attach supporting documents: It is crucial to attach any supporting documents that may strengthen your appeal. This can include medical records, test results, letters of medical necessity, invoices, and any other relevant paperwork. Make sure to label and organize the attachments appropriately.
07
Review and submit: Once you have completed the form and attached all the necessary documents, review it carefully for accuracy and completeness. Make any necessary corrections or additions before submitting it.
Who needs Amerigroup appeal form?
01
Individuals with denied claims: If your claim with Amerigroup has been denied and you believe it was unjust or incorrect, you may need to fill out the Amerigroup appeal form.
02
Policyholders or members: Any individual covered under an Amerigroup insurance policy who disagrees with a decision made by the insurance provider regarding their claim may need to utilize the appeal form.
03
Healthcare providers: In some cases, healthcare providers may also be required to fill out the Amerigroup appeal form on behalf of their patients. This can happen if they believe that a claim has been unfairly denied or if there was an error in the processing of the claim.
Fill
amerigroup reconsideration form
: Try Risk Free
People Also Ask about amerigroup second level appeal
How do I appeal Medicaid in Texas?
How do I file an appeal? If you have received a Notice of Agency Action, instructions for requesting an appeal are included on the notice. If you have not received a notice, contact 2-1-1 or visit your local office. An appeal may be requested in person, by phone, fax or mail.
How do I appeal my Amerigroup Texas provider?
You must submit your appeal within 60 days of the date on our first denial letter. You can also ask your doctor or another person to appeal for you. You can appeal in 2 ways: Call Member Services at 1-800-600-4441 (TTY 711)
What is the timely filing limit for health plan appeal?
Health insurance companies have their guidelines, and usually, the timely filing limit ranges from 30 days to 1 year from the day of service.
What is the timely filing limit for Amerigroup Medicaid Texas appeal?
You must submit your appeal within 60 days of the date on our first denial letter. You can also ask your doctor or another person to appeal for you. You can appeal in 2 ways: Call Member Services at 1-800-600-4441 (TTY 711)
What is the timely filing limit for Amerigroup IA appeal?
You or your approved representative can appeal the decision. You must file for an appeal within 60 calendar days from the time you get the Notice of Adverse Determination.
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Where do I find amerigroup appeal form nj?
It's simple with pdfFiller, a full online document management tool. Access our huge online form collection (over 25M fillable forms are accessible) and find the amerigroup appeals address in seconds. Open it immediately and begin modifying it with powerful editing options.
Can I create an electronic signature for the amerigroup texas medicaid claims mailing address in Chrome?
Yes, you can. With pdfFiller, you not only get a feature-rich PDF editor and fillable form builder but a powerful e-signature solution that you can add directly to your Chrome browser. Using our extension, you can create your legally-binding eSignature by typing, drawing, or capturing a photo of your signature using your webcam. Choose whichever method you prefer and eSign your amerigroup appeal address in minutes.
How do I complete amerigroup reconsideration form texas on an iOS device?
Install the pdfFiller app on your iOS device to fill out papers. Create an account or log in if you already have one. After registering, upload your amerigroup appeals. You may now use pdfFiller's advanced features like adding fillable fields and eSigning documents from any device, anywhere.
What is amerigroup appeal form?
The Amerigroup appeal form is a document used by members to formally dispute or appeal a decision made by Amerigroup regarding coverage, benefits, or services.
Who is required to file amerigroup appeal form?
Members of Amerigroup who disagree with a decision about their coverage or services are required to file the appeal form.
How to fill out amerigroup appeal form?
To fill out the Amerigroup appeal form, members need to provide their personal information, details of the decision being appealed, and the reasons for the appeal. It's important to follow any specific instructions included with the form.
What is the purpose of amerigroup appeal form?
The purpose of the Amerigroup appeal form is to provide members with a structured way to contest decisions related to their health care services, ensuring their concerns are formally heard and reviewed.
What information must be reported on amerigroup appeal form?
The Amerigroup appeal form must include the member's name, identification number, the date of the decision being appealed, details of the services or coverage in question, and the reasons for the appeal.
Fill out your amerigroup appeal timely filing online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Amerigroup Nj Appeal Form is not the form you're looking for?Search for another form here.
Keywords relevant to amerigroup texas appeal address
Related to amerigroup dispute form



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
